




In ETM TRT SHOM,
“Structured and Strategic Psychodynamic”
Mean . . .
pg 3 of 4



Description of ETM SHOM’s Theory of Strategic Trauma Management
ETM SHOM Applied to Systems Theory Overview
When TRT’s structure (described on page two of this section) encapsulates the etiology of trauma, and then removes it without competing with its rational, cognitive (intellectual, analytical) and behavioral effects, (which is what occurs when applying TRT to
one individual source of trauma) a manager of a trauma affected system is accorded the capacity to influence that entity the same as
the TRT clinician is the individual patient. That is, the manager of the system can remove trauma’s influences on organizational
decision making and task-based processes (just as does TRT when applied to an individual source of trauma) without disrupting that
organization’s achievement of its missions for which the entity has been constituted. That phenomenon - removing trauma’s
deleterious influences - facilitates a return to the expected management functionality lost due to the traumatic event(s) that caused the
deterioration.
Speaking analogously, ETM’s strategic function performs within systems similarly to that of laser surgery as opposed to say a general
application of an antibiotic or other medical or behavioral application to the entire entity. The goal is to remove or otherwise reverse
the individual-to-systemic etiology of trauma without disrupting the overall system’s traditional and standardized perofrmance-based
methodologies.
Where ETM SHOM provides that strategic application to both small and large systems, ETM is intended primarily for specific
entities such as individuals and families in treatment settings, crisis management organizations or those which require crisis and
trauma management responses from time to time (like school districts and military operations). SHOM is an extrapolation of ETM to
full communities such as cities and nation states. Moreover, a distinction between SHOM and ETM promotes the former as a
defensive tool intended for strengthening a nation’s security against the use of terrorism by an adversary wherein that use is intended
to weaken that security.
ETM SHOM’s Systemic Intervention on Trauma’s Destabilizing Managerial Effects
Regardless of the size and make up of the system affected by trauma, TRT ETM SHOM supports systemic interventions on trauma at
multiple levels.
1.
Perpetrator-to-target; strategically expnnging, reversing or otherwise removing trauma etiology applied as an offensive trauma
management weapon by, say, an entity which perpetrates trauma for the purpose of controlling or also adversely influencing
the decision making (for example, to destabilize a targeted polity and its management) of the targeted program, is intended and
can have the effect of interceding on that planned perpetratoor manipulative application. That is, TRT-restored identity of the
trauma-affected targets (at incremental individual levels) intercedes the controls otherwise intended by, say, a terrorist when
implementing offensive trauma.
2.
Reversing trauma at an attacked system’s incremental levels tends to facilitate reversal of systemic trauma etiology and the
quashing/ending of hysterical system member responses that tend to (pathognomonically) support the perpetrator(s) who is
(are) contriving and introducing (making ) the assaults (trauma causing and thus managerially disruptive events) for the
purpose of destabilizing the targeted polity and its management.
competing with its rational, cognitive (intellectual, analytical) and behavioral effects, (which is what occurs when applying TRT to
one individual source of trauma) a manager of a trauma affected system is accorded the capacity to influence that entity the same as
the TRT clinician is the individual patient. That is, the manager of the system can remove trauma’s influences on organizational
decision making and task-based processes (just as does TRT when applied to an individual source of trauma) without disrupting that
organization’s achievement of its missions for which the entity has been constituted. That phenomenon - removing trauma’s
deleterious influences - facilitates a return to the expected management functionality lost due to the traumatic event(s) that caused the
deterioration.
Speaking analogously, ETM’s strategic function performs within systems similarly to that of laser surgery as opposed to say a general
application of an antibiotic or other medical or behavioral application to the entire entity. The goal is to remove or otherwise reverse
the individual-to-systemic etiology of trauma without disrupting the overall system’s traditional and standardized perofrmance-based
methodologies.
Where ETM SHOM provides that strategic application to both small and large systems, ETM is intended primarily for specific
entities such as individuals and families in treatment settings, crisis management organizations or those which require crisis and
trauma management responses from time to time (like school districts and military operations). SHOM is an extrapolation of ETM to
full communities such as cities and nation states. Moreover, a distinction between SHOM and ETM promotes the former as a
defensive tool intended for strengthening a nation’s security against the use of terrorism by an adversary wherein that use is intended
to weaken that security.
ETM SHOM’s Systemic Intervention on Trauma’s Destabilizing Managerial Effects
Regardless of the size and make up of the system affected by trauma, TRT ETM SHOM supports systemic interventions on trauma at
multiple levels.
1.
Perpetrator-to-target; strategically expnnging, reversing or otherwise removing trauma etiology applied as an offensive trauma
management weapon by, say, an entity which perpetrates trauma for the purpose of controlling or also adversely influencing
the decision making (for example, to destabilize a targeted polity and its management) of the targeted program, is intended and
can have the effect of interceding on that planned perpetratoor manipulative application. That is, TRT-restored identity of the
trauma-affected targets (at incremental individual levels) intercedes the controls otherwise intended by, say, a terrorist when
implementing offensive trauma.
2.
Reversing trauma at an attacked system’s incremental levels tends to facilitate reversal of systemic trauma etiology and the
quashing/ending of hysterical system member responses that tend to (pathognomonically) support the perpetrator(s) who is
(are) contriving and introducing (making ) the assaults (trauma causing and thus managerially disruptive events) for the
purpose of destabilizing the targeted polity and its management.
competing with its rational, cognitive (intellectual, analytical) and behavioral effects, (which is what occurs when applying TRT to
one individual source of trauma) a manager of a trauma affected system is accorded the capacity to influence that entity the same as
the TRT clinician is the individual patient. That is, the manager of the system can remove trauma’s influences on organizational
decision making and task-based processes (just as does TRT when applied to an individual source of trauma) without disrupting that
organization’s achievement of its missions for which the entity has been constituted. That phenomenon - removing trauma’s
deleterious influences - facilitates a return to the expected management functionality lost due to the traumatic event(s) that caused the
deterioration.
Speaking analogously, ETM’s strategic function performs within systems similarly to that of laser surgery as opposed to say a general
application of an antibiotic or other medical or behavioral application to the entire entity. The goal is to remove or otherwise reverse
the individual-to-systemic etiology of trauma without disrupting the overall system’s traditional and standardized perofrmance-based
methodologies.
Where ETM SHOM provides that strategic application to both small and large systems, ETM is intended primarily for specific
entities such as individuals and families in treatment settings, crisis management organizations or those which require crisis and
trauma management responses from time to time (like school districts and military operations). SHOM is an extrapolation of ETM to
full communities such as cities and nation states. Moreover, a distinction between SHOM and ETM promotes the former as a
defensive tool intended for strengthening a nation’s security against the use of terrorism by an adversary wherein that use is intended
to weaken that security.
ETM SHOM’s Systemic Intervention on Trauma’s Destabilizing Managerial Effects
Regardless of the size and make up of the system affected by trauma, TRT ETM SHOM supports systemic interventions on trauma at
multiple levels.
1.
Perpetrator-to-target; strategically expnnging, reversing or otherwise removing trauma etiology applied as an offensive trauma
management weapon by, say, an entity which perpetrates trauma for the purpose of controlling or also adversely influencing
the decision making (for example, to destabilize a targeted polity and its management) of the targeted program, is intended and
can have the effect of interceding on that planned perpetratoor manipulative application. That is, TRT-restored identity of the
trauma-affected targets (at incremental individual levels) intercedes the controls otherwise intended by, say, a terrorist when
implementing offensive trauma.
2.
Reversing trauma at an attacked system’s incremental levels tends to facilitate reversal of systemic trauma etiology and the
quashing/ending of hysterical system member responses that tend to (pathognomonically) support the perpetrator(s) who is
(are) contriving and introducing (making ) the assaults (trauma causing and thus managerially disruptive events) for the
purpose of destabilizing the targeted polity and its management.
ETM TRT Strategic Theory (found in these pages three and four) Components
1.
Description of ETM SHOM’s Theory of Strategic Trauma Management
2.
Assessment, Evaluation, and Strategy (plan) for addressing Single and Multiple Sources of Trauma occurring within and affecting systems.
3.
ETM TRT SHOM definition of “incremental” address, to mean resolution of individual elements, of that which causes systemic trauma etiology.
4.
Applying TRT to Near-term vs Long-Term Trauma; and strategically heading off survival responses, also called PTSD.
5.
Application of ETM TRT’s structure to the selected source(s) of trauma within the system.
6.
Summary (from 3, 4, 5 above) of ETM’s Strategic Strata as (Hypothetically) Applied in Steps A, B, C
7. Special Traumatic Etiological Influences upon Crisis Managers and their Strategic (Focused ) Address with ETM SHOM.
8. Using ETM’s SHOM’s strategic methods to intervene upon perpetrator (terrorist) aggression, hegemony, control through violence.
9. TRT’s Interactive Rules for facilitation and Giving Feedback by Group Members and Certified ETM TRT clinicians.
10. ETM TRT SHOM Etiotropically-Focused Patient, Family, Organizational Management Education.
11. The differences between applying ETM to organizations (and elements of local communities) and SHOM to nation states responsible for their
security within the Global (world of nations).
2.a
Assessment, Evaluation, and Strategy (combining
trauma’s address with TRT’s application) for addressing
Single and Multiple Sources of Trauma and their effects
on Systems
ETM utilizes assessment and evaluation psych-socials supporting
standardized government and JCAHO audited documentation to
determine the condition to be addressed. When the information provided
by the evaluation data connotes or asseverates the presence of traumatic
etiology(s) and its prospective causes, which may present from exposure
to Alcoholism, drug addiction, homicide survival, sexual assault, other
violent crimes, combat, accident, natural disaster, life with a pathological
drug user manifesting aberrant behavior, and etcetera, that trauma
etiology ‘s address is then incorporated into the treatment plan.
Quite often, an individual will have been affected by more than one cause
of trauma. That occurrence in ETM TRT SHOM parlance is called
Multiple Sources of trauma. Recently (the last two decades), the field of
psychology has coined the phrase “complex trauma” in addressing
similar and identical conditions. Where the explanations in this section
1.b provide more definition of this phenomenon and its relationship to
ETM TRT SHOM’s structured approach, the ETM TRT Tutorial
addresses the matter and application of the referenced structure in detail.
For a quick overview, when more than one source of trauma exists, all
five phases of TRT are applied to one source at a time and until the
etiology comprising that source is reversed. Following the formula for
addressing multiple sources, TRT's five phases are then applied to any
additional sources, but almost always one source at a time. Clients
usually exit therapy for a while, however, between the address of the
sources. See 1.b for more clarification of Multiple Sources of Trauma.
trauma’s address with TRT’s application) for addressing
Single and Multiple Sources of Trauma and their effects
on Systems
ETM utilizes assessment and evaluation psych-socials supporting
standardized government and JCAHO audited documentation to
determine the condition to be addressed. When the information provided
by the evaluation data connotes or asseverates the presence of traumatic
etiology(s) and its prospective causes, which may present from exposure
to Alcoholism, drug addiction, homicide survival, sexual assault, other
violent crimes, combat, accident, natural disaster, life with a pathological
drug user manifesting aberrant behavior, and etcetera, that trauma
etiology ‘s address is then incorporated into the treatment plan.
Quite often, an individual will have been affected by more than one cause
of trauma. That occurrence in ETM TRT SHOM parlance is called
Multiple Sources of trauma. Recently (the last two decades), the field of
psychology has coined the phrase “complex trauma” in addressing
similar and identical conditions. Where the explanations in this section
1.b provide more definition of this phenomenon and its relationship to
ETM TRT SHOM’s structured approach, the ETM TRT Tutorial
addresses the matter and application of the referenced structure in detail.
For a quick overview, when more than one source of trauma exists, all
five phases of TRT are applied to one source at a time and until the
etiology comprising that source is reversed. Following the formula for
addressing multiple sources, TRT's five phases are then applied to any
additional sources, but almost always one source at a time. Clients
usually exit therapy for a while, however, between the address of the
sources. See 1.b for more clarification of Multiple Sources of Trauma.
2.b
What are “Sources” and thus “Multiple Sources” of
trauma?
In the ETM TRT SHOM lexicon, a source of trauma refers to the
trauma’s cause. The source can consists of one to numerous incidents of
trauma causing behavior. For example, life with a pathologically drug (to
include alcohol) using spouse, parent, sibling or child will produce a
single source of trauma. Many events stemming from the drug induced
aberrant activity will likely present within and from that source. A source
of trauma can also be comprised of a single event, for example, as occurs
from the homicide of a loved one.
Under the ETM formula for addressing multiple sources, TRT applies to
all the events comprising a single source before addressing another
source. That formula assigns, as a rule, the TRT clinical address to the
most recently occurring source, then in declining order until all sources
are addressed.
When a professional studies ETM Multiple Sources theory and
methodology, one finds that it allows for variances in the order and
symmetry of the TRT applications. For example, when a dramatic event
from one source of trauma, as occurs with the death of a loved, or
physical harm to the patient presented during a combat episode, the
exigency is managed under the provision of the “Most Pressing Trauma”,
anachronized as the “MPT,” methodology.
Bringing order to the address of the occurrences of multiple sources of
trauma is a fundamental requisite of ETM TRT SHOM’s structure. It is
mandatory for facilitating a consistent, congruent, and complete
conclusion to the trauma’s resolution (cure).
trauma’s cause. The source can consists of one to numerous incidents of
trauma causing behavior. For example, life with a pathologically drug (to
include alcohol) using spouse, parent, sibling or child will produce a
single source of trauma. Many events stemming from the drug induced
aberrant activity will likely present within and from that source. A source
of trauma can also be comprised of a single event, for example, as occurs
from the homicide of a loved one.
Under the ETM formula for addressing multiple sources, TRT applies to
all the events comprising a single source before addressing another
source. That formula assigns, as a rule, the TRT clinical address to the
most recently occurring source, then in declining order until all sources
are addressed.
When a professional studies ETM Multiple Sources theory and
methodology, one finds that it allows for variances in the order and
symmetry of the TRT applications. For example, when a dramatic event
from one source of trauma, as occurs with the death of a loved, or
physical harm to the patient presented during a combat episode, the
exigency is managed under the provision of the “Most Pressing Trauma”,
anachronized as the “MPT,” methodology.
Bringing order to the address of the occurrences of multiple sources of
trauma is a fundamental requisite of ETM TRT SHOM’s structure. It is
mandatory for facilitating a consistent, congruent, and complete
conclusion to the trauma’s resolution (cure).
2.a and 2.b
ETM TRT SHOM First Strategic Element - ETM Assessment and Strategy
Assessment, Evaluation, and Strategy (plan) for addressing Single and Multiple Sources of Trauma occurring within a System
[Taken (reprinted for emphasis) from page 2 of this section
Introduction and Overview
(Outline)
1.
Description of ETM TRT SHOM’s
“Strategic” Theory Elements
3.
ETM TRT SHOM Definition of “Incremental” Address, to mean Resolution of
Individual Elements, of that which Causes or Instantiates Systemic Trauma Etiology.
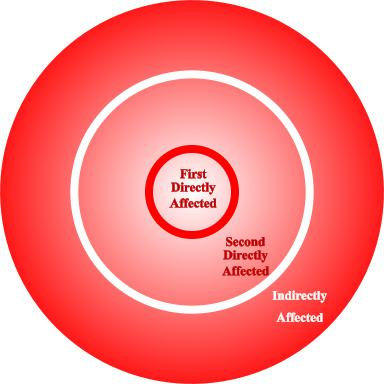
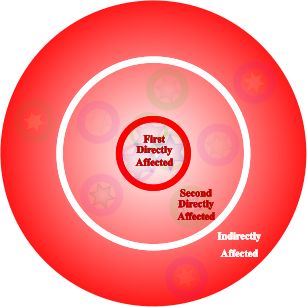
Figure 1
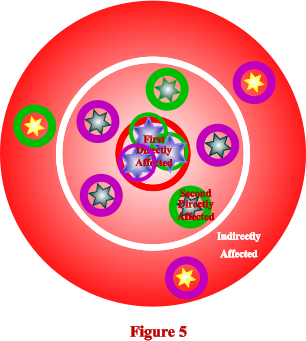
As the old trope goes, when a rock is thrown into a pond, ripples
emanate from the location where the rock impacts the water. Near the
impact, the ripples are large. They decrease in size, however, as they
move away from the center. So goes trauma etiology within a system,
referring in this discussion to a famiy, organization, local community
or nation of people. Step One frames into a management modality
procedures for evaluating, categorizing and consolidating the rippling
effect of trauma etiology, otherwise noted as the sundering of
existential identity. Thus the step (A) renders the formerly appearing-
to-be entropic or chaotic process to be orderly and manageable. Here
(below in this overview) are a few terrorism and non-combat related
examples:
emanate from the location where the rock impacts the water. Near the
impact, the ripples are large. They decrease in size, however, as they
move away from the center. So goes trauma etiology within a system,
referring in this discussion to a famiy, organization, local community
or nation of people. Step One frames into a management modality
procedures for evaluating, categorizing and consolidating the rippling
effect of trauma etiology, otherwise noted as the sundering of
existential identity. Thus the step (A) renders the formerly appearing-
to-be entropic or chaotic process to be orderly and manageable. Here
(below in this overview) are a few terrorism and non-combat related
examples:
Strategically and Incrementally Addressing Trauma with ETM TRT SHOM
is Administered (facilitated) in Several Steps. They include A, B, and C as shown below
Figure 1
Step A: Evaluate for concentric influences on the polity (citizenry) by proximity and role, respectively, to and
within an event (an attack); accordingly, schedule its affected members for (the Etiotropic) address with its
structured individual implementation with TRT into the framework shown in figure 1 and described in the
adjacent text.
within an event (an attack); accordingly, schedule its affected members for (the Etiotropic) address with its
structured individual implementation with TRT into the framework shown in figure 1 and described in the
adjacent text.




First Directly Affected
People most directly impacted by the traumatic event. A person who
1.
survives an attack where the others of his or her group (or team in combat) have been killed;
2.
survives an attack and is wounded (physically harmed or otherwise affected);
3.
is parent or sibling of a person who has been killed in an attack, other kind of homicide or accident;
4.
observes his or her very close friend or associate being killed in an attack, accident or other kind of homicide;
5.
both survives and who observes a death occur as a result of an event;
6.
has been hit by a car, and who survives, suffering both physical and psychological trauma.
Sample event: Terrorists attack a small institution.
Second Directly Affected
Similar to directly affected, but slightly farther removed from the event's impact. Examples:
1.
first responders (like Corpsmen, medics, field trauma managers) who come to the scene and participate in management of
carnage;
2.
teacher observes an accident where a child is killed, but has not known or otherwise been involved with the deceased;
3.
a person who is told of a close friend's suicide;
4.
students who are told of a teacher's (who is seen as very important to the students) sudden death from accident, homicide or
suicide;
5.
managers of an entity where its employees have been attacked;
6.
media personnel attending the scene.
Indirectly Affected (Indirect)
People affected by the trauma, but even farther removed from its impact than 2nd directly affected people. Examples:
1.
classmates (but not close friends) of a student who is reported to have been killed in an accident the previous evening;
2.
a teacher who is told of a student who is killed in an accident;
3.
all counselors and other helping people who may respond to an event scene and who may help trauma victims to address
trauma's etiology and its effects, but not necessarily participate directly in management of the carnage attending the event;
4.
persons comprising the specific home (local) community in which a targeted person has been attacked, and then wounded or
killed;
5.
the general public of a nation sharing the identity of the target having been wounded or killed.
carnage;
2.
teacher observes an accident where a child is killed, but has not known or otherwise been involved with the deceased;
3.
a person who is told of a close friend's suicide;
4.
students who are told of a teacher's (who is seen as very important to the students) sudden death from accident, homicide or
suicide;
5.
managers of an entity where its employees have been attacked;
6.
media personnel attending the scene.
Indirectly Affected (Indirect)
People affected by the trauma, but even farther removed from its impact than 2nd directly affected people. Examples:
1.
classmates (but not close friends) of a student who is reported to have been killed in an accident the previous evening;
2.
a teacher who is told of a student who is killed in an accident;
3.
all counselors and other helping people who may respond to an event scene and who may help trauma victims to address
trauma's etiology and its effects, but not necessarily participate directly in management of the carnage attending the event;
4.
persons comprising the specific home (local) community in which a targeted person has been attacked, and then wounded or
killed;
5.
the general public of a nation sharing the identity of the target having been wounded or killed.
Strategically and Incrementally Restore Event-Sundered Existential Elements of Identity (cont.)
Step B. Schedule for identity restoration from near- and long-term experienced trauma.
After codifying the trauma influenced population by levels of effect, categorize them by time. There are two predominate groupings: near-
and long-term trauma. Near-term is affixed at under ninety days; apply long-term categorization to experiences that exist in a target's
memory post that (ninety days) period.
The purpose of this schedule: it codifies, even assist in determining, the prospective and better than that even probable clinical -
management application occurring in Step C (below-next). The referenced rippling effect where trauma reduces identity has a behavioral,
also called in Etiotropic terms, natural survival, influence upon the target(s). The effect, which consists of the target's behavioral change
stemming directly incrementally from the identity sundrances (depreciating changes) does not gain impetus until it passes the referenced
ending of the near-term period: again, ninety days. Consequently, the secondary impact upon the target's identity that will begin to occur
subsequent to that period's conclusion does not present. And it likely will not.
In contrast, where the time since the event exceeds the referenced number of days, the rippling effect - referring to those codified in Step A -
upon identity begins to develop survival, also called behavioral responses to the identity changes caused by the event. Although natural and
necessary survival defenses, they also will have a secondary effect on existential (core as in must-haves) aspects of identity. Those
additional changes will all be linked as a single sequela to the first impact-depreciation. Hence, to achieve the management goals directing
this approach, the long-term trauma identification is necessary to guide the responding trauma management system to address the entire
sequela.
But those survival responses, in the DSM and other codifications, referred to as symptoms of PTSD can be quieted as in ended, but not
behaviorally, didactically or through the application of other similarly cognitive - Nosotropic (symptom-focused) approaches to trauma
management. Significantly, it doesn't matter whether or not a trauma is addressed in the long- or near-time in terms of efficiency and
thoroughness, effective address can and will occur depending on the application referenced in Step C (below). However, once system
implementers learn what's going on with trauma that is not addressed in the Nosotropic approach the interest shifts to addressing it
Etiotropically, which interprets to addressing trauma's existential identity effects sooner rather than later. Effective (Etiotropic) address of
this process is overviewed, delineated, or distinguished from what doesn't fit or work in the next subsection, Step C.
After codifying the trauma influenced population by levels of effect, categorize them by time. There are two predominate groupings: near-
and long-term trauma. Near-term is affixed at under ninety days; apply long-term categorization to experiences that exist in a target's
memory post that (ninety days) period.
The purpose of this schedule: it codifies, even assist in determining, the prospective and better than that even probable clinical -
management application occurring in Step C (below-next). The referenced rippling effect where trauma reduces identity has a behavioral,
also called in Etiotropic terms, natural survival, influence upon the target(s). The effect, which consists of the target's behavioral change
stemming directly incrementally from the identity sundrances (depreciating changes) does not gain impetus until it passes the referenced
ending of the near-term period: again, ninety days. Consequently, the secondary impact upon the target's identity that will begin to occur
subsequent to that period's conclusion does not present. And it likely will not.
In contrast, where the time since the event exceeds the referenced number of days, the rippling effect - referring to those codified in Step A -
upon identity begins to develop survival, also called behavioral responses to the identity changes caused by the event. Although natural and
necessary survival defenses, they also will have a secondary effect on existential (core as in must-haves) aspects of identity. Those
additional changes will all be linked as a single sequela to the first impact-depreciation. Hence, to achieve the management goals directing
this approach, the long-term trauma identification is necessary to guide the responding trauma management system to address the entire
sequela.
But those survival responses, in the DSM and other codifications, referred to as symptoms of PTSD can be quieted as in ended, but not
behaviorally, didactically or through the application of other similarly cognitive - Nosotropic (symptom-focused) approaches to trauma
management. Significantly, it doesn't matter whether or not a trauma is addressed in the long- or near-time in terms of efficiency and
thoroughness, effective address can and will occur depending on the application referenced in Step C (below). However, once system
implementers learn what's going on with trauma that is not addressed in the Nosotropic approach the interest shifts to addressing it
Etiotropically, which interprets to addressing trauma's existential identity effects sooner rather than later. Effective (Etiotropic) address of
this process is overviewed, delineated, or distinguished from what doesn't fit or work in the next subsection, Step C.
4.
Applying TRT to Near-term vs Long-Term Trauma; and
where applicable strategically heading off survival responses, also called PTSD.
Strategically and Incrementally Restore Event-Sundered Existential Elements of Identity (cont.)
Step C: Expected TRT Application Times given the Variables Referenced in A and B (above).
Introduction
Using the Structure described in page 2 of this Overview, Apply either TRT’s short or full (five phases) form, depending on whether the
trauma is near- or long-term, to each source of trauma caused by the event(s) to each influenced, depending on whether those persons
have been first directly-, second directly-, or indirectly-affected by the event. That application will incrementally expunge not only
individual trauma etiology caused by that event, but initiate the process of removing all that trauma’s systemic etiology as well.
Expected Application Times to Achieve Trauma’s complete Resolution given the Variables in A and B (above).
1.
Applying TRT’s short form to near-term trauma etiology can take as little as thirty minutes in only one private session, or as
much as forty-five minutes in each of several sessions. The closer the codification falls into the circle (figure 1 above) that reflects
degree of influence by the event, the more sessions that should be used to implement the short form. In catastrophic trauma
causing events, the written components of the full TRT application pertaining to the initial etiology’s sequelae (TRT Phases One
and Two) and combined with the writing element, may be valuable to achieve complete resolution.
2.
Applying TRT’s full five phases combined writing and oral methodology can take as short as three or as long as nine months to
achieve complete resolution.
Introduction
Using the Structure described in page 2 of this Overview, Apply either TRT’s short or full (five phases) form, depending on whether the
trauma is near- or long-term, to each source of trauma caused by the event(s) to each influenced, depending on whether those persons
have been first directly-, second directly-, or indirectly-affected by the event. That application will incrementally expunge not only
individual trauma etiology caused by that event, but initiate the process of removing all that trauma’s systemic etiology as well.
Expected Application Times to Achieve Trauma’s complete Resolution given the Variables in A and B (above).
1.
Applying TRT’s short form to near-term trauma etiology can take as little as thirty minutes in only one private session, or as
much as forty-five minutes in each of several sessions. The closer the codification falls into the circle (figure 1 above) that reflects
degree of influence by the event, the more sessions that should be used to implement the short form. In catastrophic trauma
causing events, the written components of the full TRT application pertaining to the initial etiology’s sequelae (TRT Phases One
and Two) and combined with the writing element, may be valuable to achieve complete resolution.
2.
Applying TRT’s full five phases combined writing and oral methodology can take as short as three or as long as nine months to
achieve complete resolution.
5.
Applying TRT to Near-term vs Long-Term Trauma; and
where applicable, strategically heading off survival responses, also called PTSD.
Step A
Step B
Step C

Near-Term Trauma

6.
Summary (from 3, 4, 5 above) of ETM’s Strategic Strata as (Hypothetically) Applied in Steps A, B, C
Strategically and Incrementally Restore Event-Sundered Existential Elements of Identity (Summary)
Evaluated to the date Step C
is to be applied




Second
Directly
Affected
Indirectly
Affected

First
Affected
Directly









Second
Directly
Affected
Indirectly
Affected
First
Affected
Directly









Appearance at six to nine months following
TRT’s completion as applied to this source of
trauma; in keeping with the model’s goal of
complete resolution the residue will be gone
within six to eighteen months.
TRT’s completion as applied to this source of
trauma; in keeping with the model’s goal of
complete resolution the residue will be gone
within six to eighteen months.


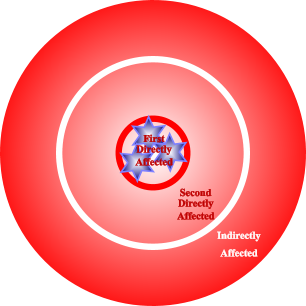
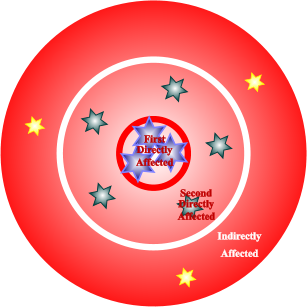
Figure 2


Near-Term Trauma

Long-Term Trauma
Evaluated to the date Step C is to be
applied
Appearance at six to nine months following TRT’s
completion as applied to this source of trauma; the
residue will be gone within six to eighteen months
completion as applied to this source of trauma; the
residue will be gone within six to eighteen months
Following this sample event, three individuals
from the affected population are evaluated and
represented (figure 2) in the innermost
categorization - as First Directly Affected - with
an equal number of larger blue stars. They are
exemplified here as
1.
A spouse of an individual killed at the
scene.
2.
A wounded civilian survivor of the attack.
3.
A police officer who witnesses her partner’s
(associate) being killed.
from the affected population are evaluated and
represented (figure 2) in the innermost
categorization - as First Directly Affected - with
an equal number of larger blue stars. They are
exemplified here as
1.
A spouse of an individual killed at the
scene.
2.
A wounded civilian survivor of the attack.
3.
A police officer who witnesses her partner’s
(associate) being killed.
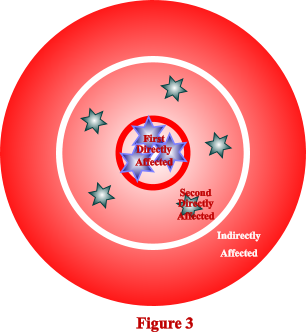
From the same sample event, five individuals
from the affected population are represented
(figure 3) in the middlemost categorization - as
Second Directly Affected - with an equal number
of medium sized green stars. The icons (green
stars) exemplify here
1.
A manager of the institution, but who was
not present during the event.
2.
An EMS worker who addresses the carnage
created by the event.
3.
A close friend, but who was not present
during the attack, of one of the deceased.
4.
A first responder (police officer) who
secures the scene subsequent to the attack
and its conclusion.
5.
A representative of the media which is
covering the event.
from the affected population are represented
(figure 3) in the middlemost categorization - as
Second Directly Affected - with an equal number
of medium sized green stars. The icons (green
stars) exemplify here
1.
A manager of the institution, but who was
not present during the event.
2.
An EMS worker who addresses the carnage
created by the event.
3.
A close friend, but who was not present
during the attack, of one of the deceased.
4.
A first responder (police officer) who
secures the scene subsequent to the attack
and its conclusion.
5.
A representative of the media which is
covering the event.
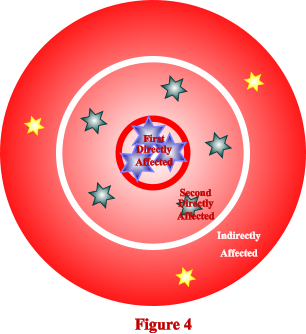
From the same sample event, thee individuals
from the affected population are represented
(figure 4) in the outermost categorization - as
Indirectly Affected - with an equal number of
smaller sized yellow stars. The icons (yellow stars)
exemplify here
1.
A trauma manager who has come to the
scene to evaluate the event’s effects upon
the participants.
2.
A chaplain who, over the subsequent time
post event, listens to those involved and
their families when they are addressing the
event.
3.
A former member of the institution who
knew the facility, organization, and
individual members, but not those who were
killed or wounded.
from the affected population are represented
(figure 4) in the outermost categorization - as
Indirectly Affected - with an equal number of
smaller sized yellow stars. The icons (yellow stars)
exemplify here
1.
A trauma manager who has come to the
scene to evaluate the event’s effects upon
the participants.
2.
A chaplain who, over the subsequent time
post event, listens to those involved and
their families when they are addressing the
event.
3.
A former member of the institution who
knew the facility, organization, and
individual members, but not those who were
killed or wounded.
Evaluate for trauma etiology by proximity and
role, to and within an event; schedule its
affected members for address with its
structured individual implementation (TRT).
role, to and within an event; schedule its
affected members for address with its
structured individual implementation (TRT).
Strategic





Strategic


Copyright 1979-2012
Jesse W. Collins II
Components one through six of this outline are found on this page three.
Components seven through eleven of this outline are found on page four.

TRT ETM and SHOM combine to provide a Structured and Strategic Psychodynamic approach to the treatment
and management of psychological trauma and PTS for both single and multiple sources of trauma affecting
individuals and systems. The first page in this section introduces, chronicles and distinguishes the more than thirty
year history of this approach. Page two overviews the “structural” component as applied to individuals. Pages
three and four summarize the “strategic” element as it is applied to systems.
and management of psychological trauma and PTS for both single and multiple sources of trauma affecting
individuals and systems. The first page in this section introduces, chronicles and distinguishes the more than thirty
year history of this approach. Page two overviews the “structural” component as applied to individuals. Pages
three and four summarize the “strategic” element as it is applied to systems.